We Keep Studying Barriers. Why Doesn’t Implementation Get Easier?
Implementation science has become remarkably good at describing why change is difficult. Over the past four decades, researchers have interviewed clinicians, observed organizations, synthesized evidence, developed implementation frameworks, and published hundreds of thousands of papers documenting the obstacles to putting evidence into practice. Leadership matters. Resources matter. Organizational culture matters. Training, workflow, stakeholder engagement, incentives, and policy all matter.
But after spending years reading this literature, I found myself asking a question that seemed strangely absent from the field itself:
Has all of this work actually made implementation easier? That question became much larger than I expected.
Over the next several weeks, I’m going to use large-scale text analysis, natural language processing, and bibliometric methods to examine nearly 1.5 million PubMed-indexed implementation publications spanning 1980 through 2025. Rather than reviewing individual studies, I’ll be looking at the literature as a whole. How has it changed? What ideas dominate it? What kinds of evidence does it produce? Most importantly, does it generate knowledge that actually helps people make implementation decisions?
This series accompanies a fully reproducible technical report. Every figure, analysis, and line of code is openly available.
The essays themselves are intentionally different from the technical report. Instead of focusing on statistical models and methods, they ask a broader question: What has implementation science become, and where should it go next?
We Keep Studying Barriers. Why Doesn’t Implementation Get Easier?
Imagine you’re responsible for implementing a new evidence-based program.
You search the literature looking for guidance. Within minutes, you find hundreds of papers explaining why implementations succeed or fail. Leadership. Communication. Resources. Workflow. Organizational culture. Stakeholder engagement. Every paper identifies important challenges, and many conclude with similar recommendations: strengthen leadership, improve communication, engage stakeholders, allocate resources.
By the twentieth paper, however, an uncomfortable realization begins to emerge.
None of them tells you what to do first.
That paradox is what motivated this project.
Implementation science has devoted decades to understanding why evidence fails to become routine practice. The field has produced sophisticated theories, rigorous qualitative research, and an extraordinary understanding of organizational complexity. Yet hospitals still struggle to sustain evidence-based programs. Schools still abandon effective interventions after grant funding ends. Community organizations continue to wrestle with staffing shortages, competing priorities, and unstable funding. Public health agencies still struggle to scale innovations amid constantly changing political and financial conditions.
If implementation science has become so much better at understanding implementation, why does implementation still seem so difficult?
To begin answering that question, I stepped back from individual papers and looked at the field itself.
The corpus I assembled contains 1,493,631 PubMed-indexed, implementation-relevant publications from 1980 to 2025. It is large enough to ask questions that are impossible to answer by reading individual studies.
Across the entire corpus, 1,457,040 publications, 97.6% of everything I analyzed, contained broad barriers-and-facilitators language. Words such as barriers, facilitators, challenges, constraints, drivers, determinants, and bottlenecks have become almost universal within implementation research.
That doesn’t mean every paper is, in a formal sense, a “barriers and facilitators” study. Quite the opposite. The explicit phrase “barriers and facilitators” appeared in only 14,301 papers, representing 0.96% of the entire corpus.
That distinction is important.
It suggests that barriers and facilitators are no longer simply one research methodology among many. They have become the dominant language through which implementation problems are discussed. The field has become extraordinarily fluent in describing obstacles.
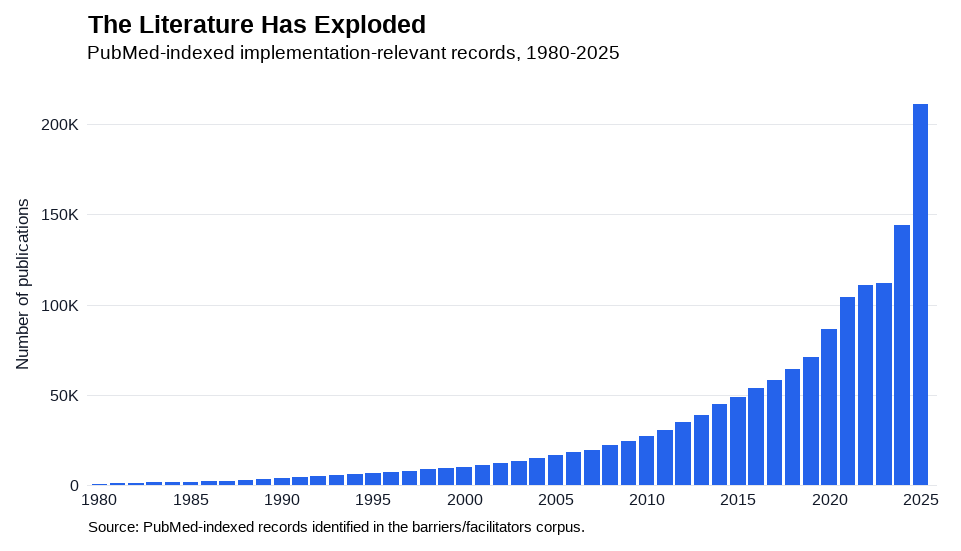
Figure 1. The literature has exploded. Annual publication counts for the implementation-relevant corpus, 1980–2025.
The second observation is impossible to miss once you plot the publication counts.
In 1980, the corpus contained just 1,022 publications. By 2025, that number had grown to 210,908—a remarkable 206-fold increase. What began as a relatively small area of inquiry has become one of the fastest-growing bodies of literature in health services research.
Viewed one way, this is exactly what scientific progress should look like. More researchers ask more questions, generate more evidence, and collectively improve our understanding of complex problems.
But another interpretation is harder to ignore.
If implementation research has expanded more than 200-fold, why do implementation leaders still describe the same struggles? Programs stall. Staff leaves. Funding disappears. Policies shift. New initiatives lose momentum before they become routine. The challenges that motivated this literature remain remarkably familiar.
Growth in publications, by itself, does not guarantee growth in useful knowledge.
The vocabulary tells a similar story.
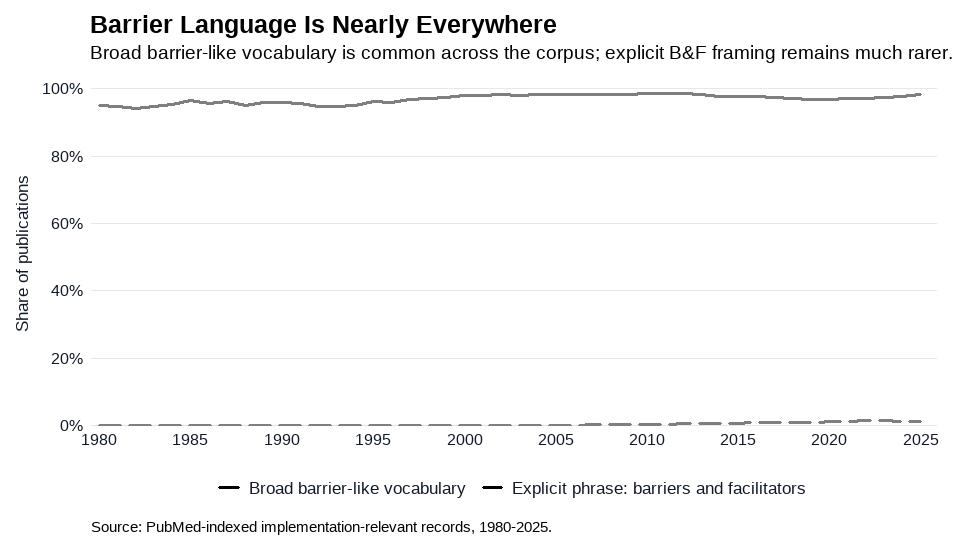
Figure 2. Broad barriers-and-facilitators language has remained nearly universal across four decades of implementation research, while the explicit “barriers and facilitators” genre has steadily emerged.
In 1980, 95.0% of publications in the corpus already contained broad barriers-and-facilitators language. By 2025, that figure had risen only slightly to 98.2%. Meanwhile, the explicit phrase barriers and facilitators grew from essentially nonexistent to appearing in 2,653 publications in 2025 alone.
The implication isn’t that implementation science became obsessed with a particular study design. Rather, it gradually adopted a common way of talking about implementation. Whether researchers were studying hospitals, schools, community organizations, or public health systems, they increasingly described implementation in terms of obstacles, enabling conditions, and organizational constraints.
There is tremendous value in that work. Barriers-and-facilitators studies have helped practitioners articulate challenges, compare experiences across settings, and identify recurring implementation problems. The field would be poorer without them.
But describing a problem and helping someone solve it are different kinds of knowledge.
A list of barriers is not a decision. A catalog of facilitators is not an implementation strategy.
Knowing that leadership, resources, communication, workflow, and organizational culture all matter doesn’t necessarily tell a health system what deserves attention next Monday morning.
That distinction is the central idea behind this series.
I’m not interested in asking whether barriers exist. Of course they do. I’m interested in asking whether implementation science has become decision-useful. Does the literature help people prioritize among competing barriers? Does it distinguish symptoms from root causes? Does it identify mechanisms rather than simply themes? Does it point toward action?
The goal isn’t to criticize barriers-and-facilitators research (maybe it is a little). It’s to understand what it has accomplished, what it still struggles to do, and what the next generation of implementation science might look like.
Because if nearly 1.5 million publications still leave implementation leaders wondering where to begin, then perhaps the next frontier isn’t discovering another barrier.
Perhaps it’s learning how to decide among the ones we already know.


