Fluoridation in U.S. Public Water Supplies: History, Science, and Debunking Myths
Community water fluoridation in the United States is a public health policy with a remarkable legacy – praised as a milestone in preventive medicine and credited with dramatically reducing dental decay, yet persistently targeted by conspiracy theories and misinformation. For over 75 years, public health and dental professionals have advocated adjusting fluoride levels in drinking water to an optimal concentration that strengthens tooth enamel and prevents cavities. This practice had* been lauded by the Centers for Disease Control and Prevention (CDC) as one of the ten great public health achievements of the 20th century.
At the same time, U.S. water fluoridation has faced vocal opposition, ranging from early Cold War-era fears of communist “mind control” plots to modern internet-fueled claims about toxicity and health risks. This article takes a straightforward, evidence-based look at water fluoridation in the U.S. It traces its history, lays out what current science says about its safety and effectiveness, and busts some common myths and conspiracy theories about fluoride.
The aim is to give a clear rundown of how fluoridation has fared over the years and set the record straight against misinformation.
The Historical Development of Water Fluoridation Policy in the U.S.
The story of fluoridation begins with a dental mystery from the early 20th century. In 1901, a young dentist named Dr. Frederick McKay opened a practice in Colorado Springs, Colorado. He was astonished to see that many locals had mottled, brown-stained teeth, a condition known at the time as “Colorado Brown Stain.” Although the staining, now recognized as dental fluorosis, was unsightly, McKay observed an interesting benefit: patients with mottled enamel had significantly fewer cavities than expected.
Over the next few decades, McKay and other researchers investigated this phenomenon. By the 1930s, the mystery was solved. The discoloration was found to be caused by very high natural fluoride levels in the local water, and this same fluoride appeared to strengthen the teeth, making them highly resistant to decay. This discovery laid the groundwork for the intentional use of fluoride as a public health tool.
The U.S. Public Health Service (USPHS) and National Institutes of Health (NIH) took great interest in McKay’s findings. Dr. H. Trendley Dean, a dental officer at the USPHS, began a series of epidemiological studies in the 1930s to pin down the ideal level of fluoride that would protect against cavities without causing fluorosis.
By 1942, after examining data from 21 cities, Dean concluded that about 1.0 part per million (ppm) of fluoride in drinking water was the optimal concentration: at or below 1.0 ppm, dental fluorosis was minimal, yet tooth decay rates were dramatically lower (in some studies, cavities occurred 50–70% less frequently in communities with ~1 ppm fluoride). Armed with this evidence, public health leaders were eager to test the benefits of raising fluoride levels in a community water supply to the optimal range.
On January 25, 1945, an important experiment began. Grand Rapids, Michigan, became the first city in the world to fluoridate its municipal water in a landmark 15-year controlled study to measure the effect of fluoride on dental caries. The fluoride level in Grand Rapids’ water was adjusted to approximately 1.0 ppm, while the neighboring city of Muskegon, with a similar population but lower natural fluoride levels, served as a comparison. Other trial pairs included Newburgh, New York (fluoridated) versus Kingston, New York (control), and a Canadian pair comparing Brantford, Ontario (fluoridated) with Sarnia, Ontario (control).
The results were striking and definitive. After just 10 to 11 years, children in Grand Rapids who had grown up drinking fluoridated water had more than 60% fewer cavities than those in the control city of Muskegon. Newburgh experienced similarly dramatic declines. By 1955, the Grand Rapids study showed a 65% reduction in tooth decay among local schoolchildren, validating fluoride as a powerful measure for cavity prevention, as noted on the historical marker pictured above.
With clear evidence supporting its benefits, fluoridation quickly transitioned from a trial initiative to an official policy. In June 1950, the American Dental Association (ADA), the U.S. Public Health Service (USPHS), and other national health organizations formally endorsed community water fluoridation and encouraged cities to implement it. At that time, the U.S. Surgeon General urged any community interested in fluoridating its water to be “strongly encouraged” to proceed. This endorsement led to widespread adoption nationwide. By the end of 1950, approximately 1.5 million Americans had access to fluoridated water; by the following year, that number rose to nearly 5 million as more cities joined the initiative. Throughout the 1950s and 1960s, the adoption of water fluoridation continued to grow steadily. Notably, New York City’s extensive water system was fluoridated in 1965. By the end of the 1960s, roughly 44% of the U.S. population served by public water systems had access to fluoridated water.
Public health authorities have framed water fluoridation as a crucial tool in the fight against one of the most widespread diseases: tooth decay. In the mid-20th century, dental caries was highly prevalent; a report from the National Institutes of Health (NIH) noted that by the 1940s, dental disease had left 3 out of 10 Americans over the age of 45 with no natural teeth. The ability to prevent cavities on a community-wide scale was celebrated as a revolutionary advancement in public health.
By 1969, the success of fluoridation was so evident that the U.S. Public Health Service established a national goal to provide fluoridated water to as many Americans as possible. Over the following decades, this objective became a standard health goal, featured in Healthy People initiatives, and the percentage of the population with access to fluoridated water continued to increase. By 2012, approximately 75% of Americans using public water supplies were receiving optimally fluoridated water. Today, over 200 million U.S. residents (about two-thirds of the total population) benefit from fluoridated tap water, a practice now common in many other countries as well.
The initiative to fluoridate water has always been grounded in the principles of prevention and health equity. Dental cavities, or caries, are more than just minor issues; they are a chronic disease that can lead to pain, tooth loss, systemic infections, and significant medical expenses. Water fluoridation was adopted as a cost-effective strategy to strengthen everyone’s teeth, regardless of age, income, or access to dental care.
Unlike other preventive measures that require individual action, such as regularly brushing with fluoride toothpaste or visiting a dentist for topical treatments, water fluoridation provides “passive” protection for the entire community. This is achieved simply by people drinking water and consuming foods prepared with it. As previously noted by the CDC, fluoridation benefits individuals “regardless of age, educational attainment, or income level,” making it especially advantageous for children in low-income families who may not receive regular dental care.
This widespread benefit, available at a low cost, has led the CDC to commend water fluoridation as “the most cost-effective method” for delivering cavity prevention to the public. Public health economists often point out that every $1 invested in water fluoridation can save approximately $20 to $50 in dental treatment costs by reducing cavities and their associated complications.
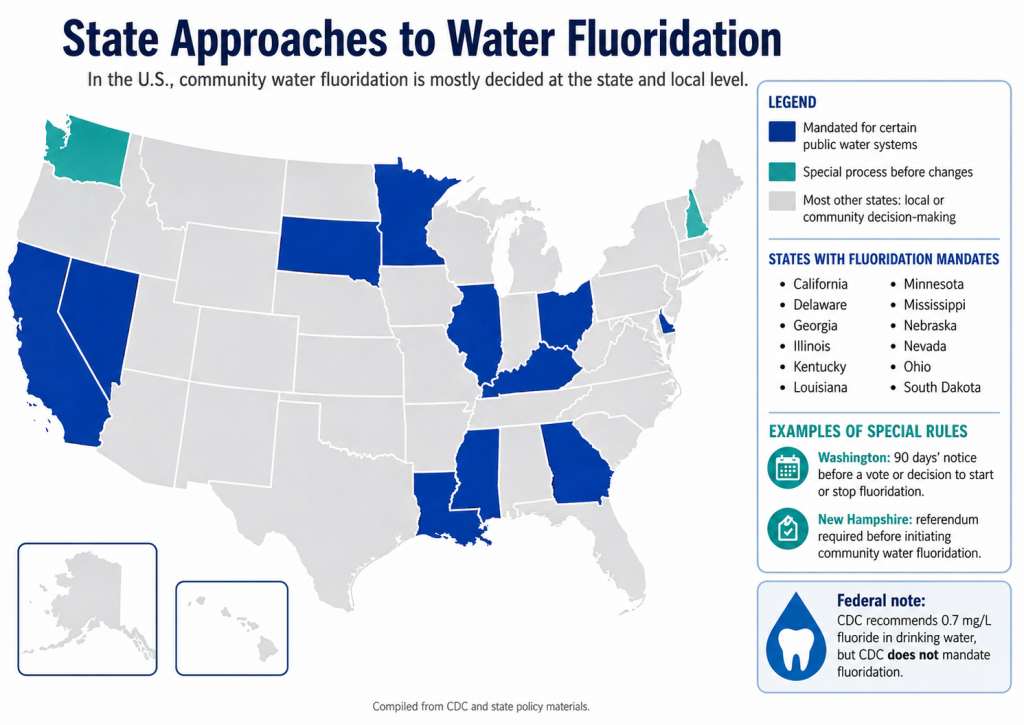
It’s worth noting that, from the beginning, public health officials approached fluoridation policy carefully. Initial endorsements in the 1940s came only after substantial research and, even then, called for continued study. Over the years, as fluoride became available from other sources (toothpastes, rinses, etc.), experts revisited the recommended water concentration to ensure maximum benefit with minimal risk. In 1962, federal guidelines set an optimal range of 0.7–1.2 ppm, depending on local climate (since people in hot climates drink more water).
By 2015, with widespread use of fluoride toothpastes and other products, the U.S. Public Health Service updated the recommendation to a single level of 0.7 mg/L (ppm) for all communities, the lower end of the old range. This level still protects dental health while avoiding excess exposure that could contribute to cosmetic fluorosis in kids. Such adjustments underscore that fluoridation policy has always aimed to strike the right balance: enough fluoride to prevent disease, but not so much as to cause harm.
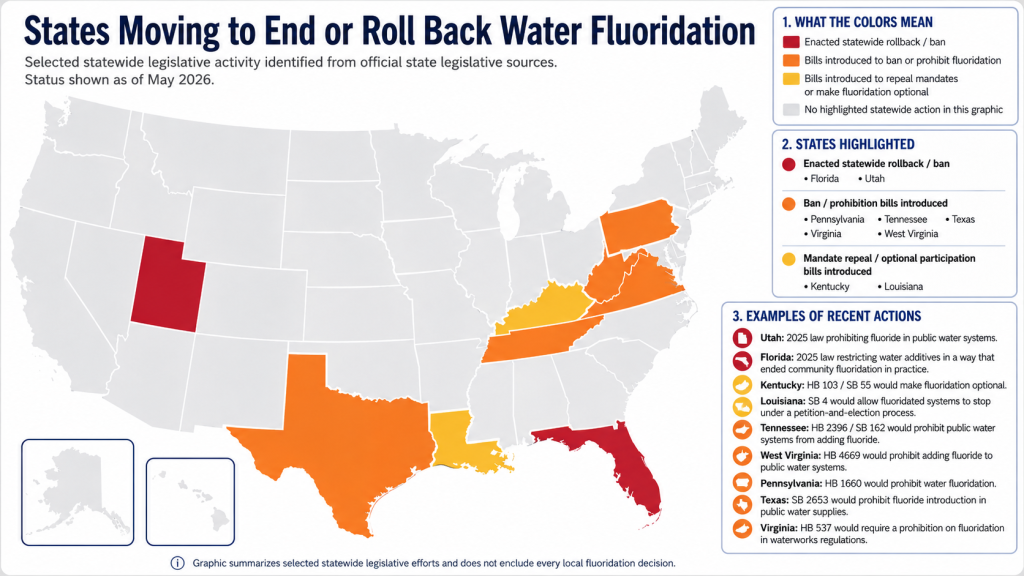
And yet, there have been legislative actions to pull this progress back.
Scientific Evidence of Fluoridation’s Safety and Effectiveness
Seven decades after the first fluoride was added to Grand Rapids’ water, the scientific verdict on water fluoridation is robust and overwhelmingly positive. Researchers have amassed an enormous body of data on two key questions:
Does fluoridation actually prevent tooth decay? And does it do so safely, without adverse health effects?
According to virtually every major health organization and rigorous review, the answer is yes: fluoridation is effective in reducing cavities and is safe at the levels used in public water systems.
Effectiveness in Preventing Dental Decay:
The anti-cavity benefits of fluoride in drinking water are well documented in both historical studies and contemporary research. In the early trials noted above, children who grew up with fluoridated water had about 50–60% less tooth decay than those who did not. These dramatic effects were repeatedly confirmed: for example, one 1950s study of 7,200 children across 21 U.S. cities found that cavities were far fewer in cities with naturally fluoridated water at around 1 ppm, and that decay rates plateaued (no further benefit) beyond about 1 ppm. The evidence was so compelling that by the late 1950s, fluoridation was hailed as a proven public health measure.
Over time, as fluoride toothpastes (introduced in the 1950s) and other topical treatments became more common, the relative advantage of water fluoridation narrowed somewhat, but it remains significant. A CDC review in 2015 estimated that fluoridated water typically reduces tooth decay rates by approximately 25% among children and adults, even in an era when people have other sources of fluoride. Public health experts emphasize that this is an average across entire populations; importantly, those with limited access to dental care or lower use of fluoride toothpaste (often in disadvantaged communities) stand to gain even more from water fluoridation.
Indeed, recent real-world data have reinforced fluoride’s impact. For instance, when the city of Calgary, Canada, ceased fluoridation in 2011, childhood cavity rates increased significantly compared with still-fluoridated Edmonton. Similarly, after Juneau, Alaska, stopped fluoridating in 2007, dental decay in children spiked, according to follow-up studies. These natural experiments echo the original trials – remove fluoride, and tooth decay rises.
In short, there is broad scientific consensus that fluoridation confers meaningful protection against cavities, reducing both the prevalence and severity of decay across communities.
From a biological standpoint, the efficacy of fluoride is well-understood. Fluoride in drinking water (and in toothpaste) helps remineralize enamel by incorporating into the tooth’s crystal structure as fluorapatite, which is more resistant to acid attack by decay-causing bacteria. Low levels of fluoride continuously present in saliva and dental plaque can halt or even reverse early tooth decay.
Notably, scientists now know that fluoride’s primary benefit is topical (at the tooth surface) rather than systemic; even swallowed fluoride that is incorporated into developing teeth plays a smaller role than post-eruption contact with enamel. But because drinking water frequently delivers low-dose fluoride to the mouth, it provides a constant preventive bath for teeth. This explains why fluoridated water helps adults as well as children – it’s not just about developing teeth but also about maintaining enamel strength. By preventing cavities, water fluoridation also helps avoid pain, tooth loss, dental infections, and the broader health issues linked to poor oral health (from nutrition problems to heart disease).
The bottom line from 75+ years of data: community water fluoridation significantly curbs tooth decay, and remains a cost-effective, equitable intervention to improve oral health.
Safety and Health Impacts:
No public health intervention can sustain itself for decades without intensive scrutiny of safety. Fluoridation is no exception – it has been one of the most closely studied (and debated) public health measures in history. Health agencies and independent scientists have periodically reviewed the evidence on whether long-term exposure to fluoridated water (at roughly 0.7–1.0 ppm) poses any risks. Again and again, the conclusion has been that fluoridation at recommended levels is safe for people of all ages. The U.S. CDC, the World Health Organization, the American Medical Association, the American Dental Association, and their counterparts worldwide all endorse water fluoridation as safe based on current science.
To understand safety, it’s useful to clarify dosage. The U.S. Environmental Protection Agency (EPA) sets enforceable standards for certain drinking water contaminants. For fluoride, the EPA’s regulatory maximum is 4.0 ppm, and a secondary guideline of 2.0 ppm to protect children from potential dental fluorosis. These EPA limits are far above the optimal 0.7 ppm used in fluoridation programs. The reason the EPA allows up to 4 ppm is that, in some areas, natural fluoride in groundwater reaches that level; 4 ppm was set in 1986 as a threshold to avoid serious effects (such as bone disorders), though it may cause cosmetic fluorosis.
In 2006, a committee of the National Research Council (NRC) reviewed new data. It recommended lowering the 4.0 ppm maximum, noting evidence that even 4 ppm over many years could increase risk of enamel fluorosis and slight bone weakening. Importantly, the NRC’s report did not call into question the safety of water fluoridation at ~0.7–1 ppm; in fact, the committee explicitly stated that their concerns at 4 ppm “said absolutely nothing about risk from 1 ppm” used in community fluoridation. The NRC panel looked for links to various health issues (from hormone and thyroid effects to cancer and neurological effects) and found no evidence of harm at the lower concentrations used in public water systems.
The only well-known side effect of fluoridation in the U.S. is dental fluorosis, which is mostly mild. Fluorosis refers to faint white specks or streaks on the tooth enamel of children who receive excess fluoride while their teeth are developing. In fluoridated communities, a small percentage of kids might develop very mild fluorosis (often barely noticeable white flecks) – a cosmetic issue with no impact on tooth function. Public health officials have balanced this risk by setting the optimal level low enough to minimize fluorosis while still preventing cavities. The modern prevalence of mild fluorosis also reflects cumulative fluoride intake from sources beyond water (such as toothpaste, certain teas, and dietary sources).
That’s one reason the fluoride recommendation was nudged down to 0.7 ppm in 2015 – to strike that balance. Crucially, moderate-to-severe fluorosis (with brown staining or enamel pitting) is exceedingly rare in fluoridated areas and is typically seen only where water fluoride levels are naturally very high (well above 2–3 ppm) or where children consume excessive fluoride from multiple sources. Health authorities regard the cosmetic risk of mild fluorosis as an acceptable trade-off given the far greater burden of tooth decay that fluoridation averts. Public education (such as advising parents to supervise young children’s toothpaste use and to use only a pea-sized amount) also helps reduce preventable overexposure to fluoride during childhood.
Beyond teeth and bones, what about other health outcomes? Opponents of fluoridation have long alleged links to ailments ranging from cancer to cognitive problems. These claims have been rigorously investigated.
Cancer has likely been the most thoroughly studied potential risk associated with fluoride. In the 1990s, a high-dose animal study conducted by the National Toxicology Program found an ambiguous indication that male rats given water with very high levels of fluoride had a slightly higher incidence of bone tumors (osteosarcomas) than expected. However, this result was not observed in female rats or other species, and no clear evidence that fluoride causes cancer has been found in any human population.
The American Cancer Society states that many epidemiological studies comparing cancer rates before and after fluoridation in communities, or between fluoridated and non-fluoridated areas, have shown no consistent differences in overall cancer incidence, including specific types like osteosarcoma. A review conducted by a scientific panel in California in 2011 concluded that fluoride “has not been clearly shown to cause cancer.” This conclusion is consistent with earlier reviews by the National Public Health Service and the International Agency for Research on Cancer. The consensus among expert agencies is that optimal levels of fluoridation do not pose a detectable cancer risk to humans.
In plain terms, after decades of scrutiny, no credible link between fluoridated water and cancer has been demonstrated.
Similarly, extensive research has found no proven association between fluoridation and other chronic health issues. Rates of heart disease, kidney disease, and other conditions are no higher in fluoridated communities than in non-fluoridated ones, after controlling for other factors. Opponents have pointed to laboratory studies suggesting fluoride can affect thyroid hormones or enzyme systems. Still, such effects typically occur at concentrations or doses far above those from drinking fluoridated water.
Fluoride can inhibit certain bacteria and enzymes, which helps prevent cavities. However, at the trace levels found in tap water, there is no evidence of systemic toxicity in humans. Modern reviews, including those from Australia (2016), Ireland (2002), the U.K., and the U.S. Community Preventive Services Task Force, have consistently concluded that water fluoridation is both safe and effective. The American Public Health Association (APHA) summarized this conclusion well by stating that after reviewing all major studies, “opponents have claimed potential toxicity, but studies of scientific merit have supported none of these claims.”
To illustrate the safety margin: fluoride at 0.7 ppm means 0.7 milligrams of fluoride per liter of water. A typical adult drinking 2 liters a day would ingest about 1.4 mg of fluoride – an amount that the body handles easily (half is excreted, half may incorporate into bone or teeth). Compare that to doses known to cause acute toxicity: one would have to consume hundreds of liters of fluoridated water literally at once to approach a lethal dose. As toxicologists often say, “the dose makes the poison.”
Some substances can be deadly in high quantities but harmless or even beneficial in small amounts. A common example is chlorine, which is a poisonous gas at high concentrations but serves as a lifesaving disinfectant in water at just a few parts per million. Similarly, fluoride is used in drinking water at a safe level of 0.7 ppm. The Environmental Protection Agency (EPA) has set a limit of 4 ppm, which includes a safety margin. Even at this higher level, only subtle effects, such as mild fluorosis and minor bone risks, have been observed after long-term consumption. However, at the typical levels used for water fluoridation, no adverse health effects have been identified.
This is not to suggest scientists have stopped looking; surveillance continues, and any new hypotheses (such as recent questions about fluoride and neurodevelopment) are investigated, as discussed below.
But the weight of evidence to date supports the conclusion that current fluoridation levels are not harmful to human health.
Common Conspiracy Theories and Myths About Water Fluoridation
Given the strong scientific consensus on fluoridation’s benefits and safety, it may seem surprising that the practice remains controversial in some circles. Yet water fluoridation has been dogged by opposition since its inception – often driven less by scientific debate and more by ideology, misinformation, and even wild conspiracy theories. Understanding these claims is important for public health professionals, both to address public concerns and to counteract false narratives. Below, we examine the most common myths and conspiracy theories about fluoridated water, paired with factual rebuttals from authoritative sources.
“Fluoride Is a Poison Used to Medicate or Harm the Population”
A common belief among anti-fluoride activists is that fluoride is a toxic substance being irresponsibly added to drinking water. Opponents often point out that fluoride compounds, such as sodium fluoride, have been used as active ingredients in pesticides and rat poison. They argue that the government is essentially putting “rat poison” in the water. Some even claim that fluoridation constitutes mass medication or a covert attempt to harm people.
They emphasize that fluoride is not an essential nutrient—no one suffers from a “fluoride deficiency”—implying that any addition to water is both unnecessary and dangerous. In more extreme versions of this argument, conspiracy theorists suggest that fluoridation was devised as a way for industries to dispose of toxic waste, specifically fluoride byproducts from fertilizer or aluminum factories, by diluting them in public water supplies under the guise of promoting dental health. This narrative proposes a sinister collaboration among government, industry, and even the military to “medicate” the population without consent.
Fluoride at high concentrations is indeed toxic – but so are many substances that we intentionally ingest in safe doses. The maxim “the dose makes the poison” is crucial. At the 0.7 ppm level in water, fluoride is not a poison but a beneficial trace element, akin to the chlorine used to purify water or the iodine added to table salt. To illustrate, sodium fluoride can kill a rat in one large dose, but a rat would have to drink roughly 100 liters of fluoridated water at once (without urinating) to receive a lethal amount. In other words, the concentration is so low that acute toxicity from drinking fluoridated water is essentially impossible. As for chronic exposure, regulatory agencies set limits precisely to prevent toxic accumulation – and decades of monitoring in fluoridated communities show no signs of poisoning or elevated disease rates. The only detectable effect is the aforementioned mild fluorosis in a minority of cases, which is a cosmetic nuisance rather than a “toxic” outcome.
Fluoride is naturally found in nearly all water sources, though at varying levels. The fluoridation program adjusts the fluoride concentration to an optimal level. We often consume trace chemicals that can be harmful at high doses but are harmless at low doses. For example, chlorine is intentionally added to water to kill pathogens and is significantly more acutely toxic than fluoride. However, when maintained at around 1 ppm, it makes water safe to drink without causing any negative effects. Similarly, sodium chloride (table salt) can be lethal in large quantities but is essential to our diet in small amounts.
Context is crucial: labeling fluoride a “poison” without proper context is as misleading as claiming that oxygen is toxic (which can be true at high pressure) or that morphine is a dangerous drug (it is, except when used appropriately as a painkiller). Public health interventions often involve the use of chemicals, such as water chlorination or fortifying milk with vitamin D, and in each case, whether something is harmful, harmless, or beneficial depends on the dose and its intended purpose.
The trace amounts of fluoride in drinking water are far from levels that would cause poisoning. Toxicological reviews conducted by the U.S. Agency for Toxic Substances and Disease Registry and other organizations have found no evidence that fluoridated water, when consumed at recommended levels, causes systemic toxicity in humans.
What about the “industrial waste” conspiracy – that fluoridation was a cover for dumping pollutants?
This statement distorts a historical fact. One common fluoride additive used in water (fluorosilicic acid, or its sodium salt) is indeed sourced from the phosphate fertilizer industry. During phosphate fertilizer production, fluoride compounds are captured from factory emissions to prevent environmental pollution. These captured fluorides can then be purified and sold for water treatment.
However, public health authorities did not initiate fluoridation to benefit the industry; it began because medical research demonstrated fluoride’s dental benefits. Initial trials in the 1940s used sodium fluoride supplied by chemical companies and were conducted under strict scientific oversight, rather than dumping uncontrolled waste into the water supply. After fluoridation proved effective, municipalities turned to the most cost-effective source of fluoride, which happened to be the byproduct from fertilizer plants. Importantly, this byproduct is not used in its raw, uncontrolled form; it is processed to meet stringent quality standards (AWWA/NSF International) that ensure safety and purity.
When added to water, fluorosilicic acid (H₂SiF₆) dissociates immediately, releasing fluoride ions identical to those in natural calcium fluoride. The trace levels of other substances present in these additives, such as metals, are strictly limited to well below EPA allowable levels. In fact, studies have shown that any heavy metal impurities introduced by fluoridation chemicals are so minimal that they often contribute less than what naturally occurs in typical water sources.
Both the CDC and EPA affirm that fluoridation additives are safe. The process effectively recycles a captured environmental pollutant (fluoride gas) into a public health asset, rather than allowing it to contaminate the air. Far from “mass poisoning,” this is an example of regulated industrial byproduct reuse that benefits public health. Without this source, communities would have to obtain fluoride from other chemical suppliers at a higher cost—the fluoride ion itself remains the same.
The idea that fluoridation constitutes forced medication deserves clarification. Fluoride in drinking water is similar to iodine added to salt or folic acid added to grain products—these are community-wide preventive measures. Courts in the United States have consistently rejected the argument that fluoridation infringes on individual rights or constitutes unlawful “mass medication.” For over 70 years, no U.S. court of last resort has ruled against water fluoridation on these grounds. Both state supreme courts and the U.S. Supreme Court have upheld the view that fluoridation is a reasonable public health measure rather than a violation of due process or personal liberty.
The ethical principle guiding this stance is that the government has a responsibility to protect public health, much like the accepted practice of chlorinating water to prevent cholera, even though individuals do not “consent” to the addition of chlorine. In practice, any resident who strongly opposes fluoride has personal mitigation options, such as using filters or drinking bottled water, though these alternatives come at a cost. From a public policy standpoint, the minuscule concentration of fluoride added to water is not regarded as a “drug” but rather as a fortification—a way to adjust a natural element in water to improve health, just like we adjust the pH or add other minerals for water quality.
Leading health ethics experts generally consider fluoridation comparable to other widely accepted public health interventions that provide significant benefits with minimal risk. For instance, the Irish Supreme Court explicitly ruled that water fluoridation is not mass medication but rather a health measure aimed at the common good, a view supported by many public health ethicists. Therefore, the depiction of fluoridation as a sinister form of forced drugging lacks support from legal precedent or public health ethics. The goal is to prevent disease, not to treat individuals for an illness, and the method involves adjusting an environmental exposure, much like adding vitamin D to milk to prevent rickets. The overwhelming majority of public health and medical organizations affirm that fluoridation is safe, effective, and socially beneficial, rather than a covert scheme to cause harm.
“Fluoridation Causes Cancer and Other Serious Diseases”
The Claim: Another common refrain in anti-fluoridation circles is that fluoride causes cancer, particularly bone cancer (osteosarcoma), or contributes to diseases like thyroid disorders, kidney disease, and even lowers fertility or causes Alzheimer’s. These claims often cite isolated studies or anecdotal reports. For example, opponents frequently mention a 1990 government study where fluoride was linked to osteosarcomas in male rats, or a since-debunked analysis suggesting higher bone cancer rates in some fluoridated areas. In essence, the claim is that fluoridation’s health risks are far-reaching and that it might be responsible for a host of chronic ills, despite official assurances.
Reality and Rebuttal: Extensive epidemiological research has searched for associations between fluoridated water and rates of cancer or other chronic diseases, and the vast majority of well-conducted studies find no evidence of harm.
Taking cancer as the prime example, multiple expert panels (e.g., National Public Health Service 1991, University of York 2000, National Research Council 2006, EU SCHER 2010, California CIC 2011) have reviewed all the data and concluded there is no credible link between community water fluoridation and cancer risk. The American Cancer Society summarizes that after decades of study, “the general consensus is that there is no strong evidence of a link between water fluoridation and cancer. Yes, the 1990 high-dose rat study initially raised a question, but scientists interpret those findings with caution. The term “equivocal evidence” was used because the increase in tumors was borderline and seen only in one sex of one species. Subsequent research in humans has not borne out a higher incidence of osteosarcoma in fluoridated vs. non-fluoridated communities. For instance, a carefully designed Harvard study in the 2000s (Bassin et al.) reported a possible fluoride-osteosarcoma link in young males, but a larger follow-up study including bone fluoride levels found no difference between osteosarcoma patients and controls. Large population studies in the U.S., UK, and elsewhere find no pattern of higher cancer rates correlated with fluoridation. It’s worth noting osteosarcoma is very rare (about 500 cases a year in U.S. youth), so studies need to combine many data points; when they do, the data do not show an increase attributable to fluoride.
The alleged links to other diseases are similarly unsupported when examined rigorously. For thyroid function: high doses of fluoride can affect thyroid hormone levels (fluoride was historically used to treat overactive thyroid at doses hundreds of times higher than in water), but multiple studies have found normal thyroid function in populations consuming fluoridated water. The NRC’s 2006 review noted some animal and cellular evidence of possible thyroid or endocrine effects at high exposures, but found no population-level evidence of thyroid dysfunction at 1 ppm. Kidney disease is another concern sometimes raised, because kidneys excrete fluoride, some worry that people with impaired kidneys could accumulate fluoride.
However, clinical studies have not found that fluoridation causes kidney problems in healthy people, and patients on dialysis (who receive large water exposures) are monitored under separate water-purity standards. The NRC did advise that people with severe renal impairment might retain more fluoride, but no surge in fluorosis or bone issues has been observed among dialysis patients in fluoridated regions (dialysis centers typically filter water regardless).
More broadly, research on bone health has gone back and forth on whether long-term fluoride slightly strengthens or weakens bones. Some earlier studies in high-fluoride areas suggested a small increase in hip fractures, while others showed no difference or even potential protective effects of fluoride on bone density. The latest consensus is that if fluoridation has any effect on fracture risk, it is so small as to be difficult to detect – and most evidence shows no significant difference in fracture rates between fluoridated and non-fluoridated populations. The NRC 2006 noted that at 4 ppm, there is a possible increase in bone fractures, but found no concerns at 1 ppm.
Opponents sometimes enumerate scary-sounding effects from fluoride (from infertility to brain damage). These claims often trace back to studies of regions with excessive fluoride levels far above levels used for fluoridation, or to laboratory experiments in which fluoride was applied at high concentrations to cells or rodents. For example, in parts of India and Africa with extremely high natural fluoride (e.g., 8–12 ppm in well water), crippling skeletal fluorosis and other health issues are real problems. Those cases underscore that excessive fluoride can be harmful, but they do not provide evidence against the controlled, low-dose use of fluoride. Think of it like selenium or iodine – both are essential micronutrients that can cause toxicity in excess. The presence of endemic fluorosis in some developing regions is why the WHO and others work on safe water standards and, in some cases, on defluoridation programs for sources above 1.5 ppm.
However, those scenarios bear no resemblance to the fluoridation levels in U.S. water. As for assertions like “fluoride causes Alzheimer’s” or “fluoride causes arthritis,” these are not supported by credible, peer-reviewed research. No causal link between fluoridation and neurological degenerative diseases has been established. One can find speculative papers or hypotheses (for instance, a notion that fluoride could complex with aluminum and somehow impact the brain), but epidemiological studies do not show higher dementia rates in fluoridated areas.
The weight of scientific evidence firmly indicates that fluoride at 0.7 ppm in water does not cause generalized disease.
As the APHA position paper concluded after reviewing numerous studies, none of the health effect claims by anti-fluoride groups have been substantiated by sound science.
Health professionals need to communicate that the absence of evidence of harm is based on substantial data. It’s not a case of “we haven’t looked”; it’s a case of we have looked very hard, and nothing credible or consistent has emerged. The U.S. has had fluoridation since the 1940s – multiple generations have lived in fluoridated communities. If there were a significant increase in cancer, metabolic diseases, or mortality linked to fluoride, it would have been detected in public health statistics by now. Instead, life expectancy has risen, and dental health has markedly improved.
Of course, correlation is not causation in either direction, but large epidemiological analyses show no red flags. For example, a comprehensive study by the New York State Department of Health in 1990 found no differences in cancer rates between counties with fluoridated water and those without. Internationally, reviews in countries like the UK and Australia have echoed that finding for cancers, bone health, and other outcomes.
The claim that fluoridation causes dread diseases is not supported by mainstream science. The American Cancer Society, National Cancer Institute, World Health Organization, and many others have publicly stated that there is no evidence that fluoridated water increases cancer risk. The CDC also affirms that dozens of studies have failed to link fluoride with any systemic health disorder. Public health professionals can confidently rely on these authoritative reviews when countering cancer scares or similar claims. Fluoridation’s benefits vastly outweigh any hypothetical risks, and after decades of observation, its safety profile remains solid.
“Fluoride Lowers IQ and Is a Neurotoxin (Mind Control Plot)”
The Claim: Perhaps the most dramatic conspiracy theory about fluoridation – popularized in the 1950s and enduring in various forms – is that fluoride has effects on the human brain, dulling intelligence or even controlling minds. In its most fantastical version, anti-fluoride agitators in the Cold War era claimed fluoridation was a communist or government scheme to make the populace submissive by “narcotizing” certain brain areas. This was famously satirized in Stanley Kubrick’s film Dr. Strangelove, where a deranged general rants that fluoridation is a Soviet plot to taint Americans’ “precious bodily fluids”. While few today take the “mind control” trope literally, a modern incarnation of this fear has arisen in the form of scientific studies suggesting fluoride might reduce children’s IQ or impair neurodevelopment.

Activists often cite a 2012 Harvard meta-analysis that found that children in high-fluoride areas of China had lower average IQs than those in low-fluoride areas. More recently, a 2019 study in JAMA Pediatrics reported an association between higher in utero fluoride exposure (among pregnant Canadian women) and slightly lower IQ scores in their offspring at ages 3–4. Opponents seize on these studies to argue that even the levels of fluoride used in U.S. water could be “lowering our intelligence” or harming children’s brains, thus reviving the notion that fluoride is a neurotoxin and hinting at sinister consequences.
Reality and Rebuttal: Let’s disentangle the hyperbole from the evidence. First, the “communist plot” and mind-control claims are pure conspiracy theories with no factual basis. They emerged from the fevered anti-communist atmosphere of the 1950s. Influential far-right groups like the John Birch Society spread the idea that fluoridation was a socialist scheme to weaken American public health or impose collectivist control. Needless to say, there was never any evidence for this; fluoridation was initiated by American public health officials and scientists, not communist infiltrators, and the early results clearly improved health (fewer cavities, better quality of life) rather than harmed it. Historical research shows that those early accusations were a form of fear-mongering that attached itself to a new public health program during the Red Scare. The absurdity of those claims has been widely recognized – they often serve as a cautionary tale of how propaganda can try to derail science-backed policies. The fact that a major motion picture in 1964 lampooned the fluoride conspiracy theory speaks to how far-fetched it was perceived even at the time. In short, fluoride does not make people docile or obedient, except perhaps by saving them from toothache distractions. There is absolutely no mechanism by which trace fluoride “controls minds,” and no reputable scientist would entertain that notion. It survives only as a meme or a historical footnote (and unfortunately, as an occasional talking point in fringe circles).
Now, turning to the more serious question: Does fluoride exposure affect IQ or neurodevelopment? This is an area of active research and some debate. It is true that dozens of studies, mostly from regions with endemic high fluoride levels, have found correlations between high water fluoride levels and lower cognitive scores in children. However, context is key. Many of those studies took place in rural China, India, and Mexico, in communities with fluoride levels far above 1 ppm – sometimes 2, 4, or 8 ppm or more – often coupled with poor nutrition or co-exposures (such as high arsenic) that could confound results. The Harvard review (Choi et al. 2012), which aggregated 27 such studies, concluded that children in high-fluoride areas had lower IQs by a few points on average. Still, the authors themselves cautioned that the fluoride levels were typically very high and the studies had limitations. They explicitly stated that the findings were not directly applicable to low-exposure populations receiving optimally fluoridated water (around 0.7 ppm) – further research was needed.
The 2019 Canadian study (Green et al.) was more directly relevant to community fluoridation, as it examined maternal urinary fluoride levels in cities with ~0.7 ppm fluoride vs. those without. It found a small association: roughly a 1 mg/day higher fluoride intake among pregnant women was associated with a 3-4-point lower IQ in their children (with the effect more pronounced in boys in one analysis). This study garnered media attention and raised concerns. However, scientists have pointed out numerous caveats: the IQ differences were modest, the measurement of fluoride intake was indirect (partly based on self-reported water consumption, which can be imprecise), and there were puzzling inconsistencies (such as an effect seen in boys but not in girls for one measure). The study’s own data showed that average IQ scores were the same in fluoridated vs non-fluoridated cities (108 in both); the difference emerged only after complex statistical adjustments and subset analyses, leading some experts to question the practical significance of the findings. Furthermore, critical factors such as the mother’s IQ or specific environmental exposures weren’t fully accounted for.
Follow-up studies and reviews (including a 2021 benchmark dose analysis by the National Toxicology Program) have not reached consensus, and debate continues within the research community. It’s important to note that even if there is a real effect of high fluoride on neurodevelopment, the data so far suggest it is a subtle effect (a few IQ points), nothing remotely like a dramatic “brain damage” scenario. In fact, some experts point out that any potential risk might be mitigated easily – for instance, pregnant women who are concerned can opt for filtered or bottled water during pregnancy as a precaution, which would not significantly undermine the general benefits of community fluoridation.
Leading health organizations have not changed their stance on fluoridation in light of these recent studies, but they are monitoring the research. A 2020 expert panel in Canada reviewed the evidence and reaffirmed support for fluoridation, stating that the collective evidence still indicates safety at recommended levels (while acknowledging ongoing research on neurodevelopment). The important perspective here, as articulated by Dr. Joseph Schwarcz in the McGill Office for Science and Society, is that a single study should not dictate policy – especially when the effect size is small, and causation is not established. Public health decisions rely on the bulk of evidence. And the bulk of evidence still tilts heavily in favor of fluoridation’s safety. The CDC, ADA, and WHO have continued to endorse fluoridation, citing that the alleged IQ effects are unproven and, if they exist at all, likely minor compared to the proven benefits in cavity prevention.
In summary, while the question of fluoride and IQ deserves further scientific inquiry, it is false and irresponsible to claim that fluoridation is a “mind-control plot” or that it is making the population measurably less intelligent. If that were true, one would expect to see clear cognitive deficits in fluoridated vs. non-fluoridated populations, and no such pattern has been observed in national data (for instance, overall educational performance or IQ distributions do not differ in cities on fluoridated water). Instead, we have nuanced research findings that warrant further study but do not override the decades of evidence supporting fluoridation’s safety.
Public health agencies emphasize keeping an eye on new research, but also remind us that many environmental factors can affect IQ (lead exposure, socioeconomic status, nutrition, etc.), and that fluoride at 0.7 ppm is unlikely to be a significant contributor compared with these. The conspiratorial framing of this issue – as if fluoride were intentionally added to dumb people down – has no scientific backing. It’s a modern twist on an old paranoia. Public health experts can acknowledge genuine scientific questions (like the recent fluoride/IQ studies) while strongly rejecting the hyperbole. As it stands, the best evidence indicates no neurologic or cognitive harm from optimally fluoridated water, and certainly nothing to suggest any “mind-numbing” effect that some conspiracy theorists dramatically claim.
“Most of Europe Rejects Fluoridation – That Must Mean It’s Bad or Unnecessary”
The Claim: Fluoridation skeptics often point out that many countries, especially in Western Europe, do not fluoridate their water. Only a handful of European countries (Ireland, the UK in some regions, Spain in some areas) use water fluoridation, whereas most have opted not to, or have even banned it. Opponents argue that Europe’s dental health is as good as, or even better than, the United States’, implying that fluoridation is unnecessary. They claim that Europe’s rejection of fluoridation is due to safety or ethical concerns, and use this as evidence that the U.S. is out of step or blindly continuing a flawed policy. A related claim is that tooth decay rates have fallen worldwide, including in non-fluoridated countries, due to factors such as improved hygiene and diet rather than fluoridated water. Therefore (the argument goes), why medicate the water when it’s not needed?
Reality and Rebuttal: Indeed, fluoridation policy differs internationally – but the reasons are more complex than opponents suggest, and they do not boil down to fluoridation being ineffective or dangerous. Many European countries have relatively low levels of natural fluoride in their water and, historically, did not adopt water fluoridation for a variety of practical and political reasons. Some countries, like Germany, have a highly decentralized water system with many small sources, making centralized fluoridation logistically challenging. Others, like Sweden and the Netherlands, had vigorous debates about individual rights and chose not to implement fluoridation in the 1970s, in some cases because alternative methods were in place.
Notably, Europe has embraced other forms of fluoride delivery: fluoridated table salt is common in countries such as Switzerland, France, and Germany, reaching a large share of the population. Salt fluoridation is an effective public health strategy as well – it’s essentially another way to get fluoride to people (similar to how iodized salt works for iodine). Some European nations also have extensive preventive dental care programs in schools, or naturally fluoridated water in certain regions that suffices.
Crucially, European health authorities do not generally claim that fluoridation doesn’t work or is unsafe. In fact, the European Academy of Pediatric Dentistry and other expert bodies have stated that water fluoridation is effective in reducing caries. Still, given the political climate and alternatives like salt fluoridation, many countries have chosen those routes. For example, after a comprehensive review, the UK’s Public Health authorities still support fluoridation and have been gradually expanding it regionally (Birmingham and Newcastle have had it for decades with excellent results, and more areas are now considering it). Ireland has had nationwide fluoridation since the 1960s and retains it with public support.
In short, the absence of water fluoridation in some countries is not proof of its ineffectiveness; often, it’s a result of political decisions favoring alternative methods. In terms of ethics, some countries framed fluoridation as compulsory medication and lacked the political will to push it through, but that doesn’t amount to a scientific condemnation. Indeed, in places like New Zealand and Australia, where the political climate is more similar to that of the U.S., fluoridation is widespread and strongly supported by health authorities for the same evidence-based reasons.
Regarding the decline in cavities globally: It’s true that dental decay has declined in both fluoridated and non-fluoridated countries over the last half-century. This is thanks to multiple factors, especially the advent of fluoride toothpaste (now almost universal) and improved dental care and awareness. Public health analysts acknowledge that it is harder today to detect a large difference in decay rates attributable solely to water fluoridation, because even children in non-fluoridated areas likely use fluoride toothpaste and may receive other sources of fluoride.
However, differences still exist.
When you carefully compare demographically similar populations, those with fluoridated water tend to have lower rates of cavities. For instance, one study cited earlier compared two Canadian cities (Calgary vs. Edmonton) and found that tooth decay increased in Calgary after fluoridation was stopped, whereas Edmonton (with continuing fluoridation) remained lower. Similarly, within the U.S., studies have shown that children in communities with fluoridated water have, on average, 25% fewer decayed teeth than those in communities without fluoridated water, even after controlling for socio-economic status. The CDC attributes a sizable portion of the decline in U.S. tooth decay since the 1960s directly to community water fluoridation and fluoride products.
Opponents’ use of broad WHO data comparisons has been criticized for not accounting for confounders – countries differ in diet, dental services, use of fluoride toothpaste, etc. The plateau or decline in decay in many countries likely reflects the fact that once you saturate a population with fluoride (be it in water, salt, or toothpaste) and with dental care, you reach a low baseline level of decay. Non-fluoridating countries simply took other routes to achieve the same results, often with similar fluoride reach (for instance, fluoridated salt in Europe reaches millions and has been credited with significant reductions in cavities).
So, the claim that “Europe doesn’t fluoridate and they’re fine” doesn’t capture the whole story. A more accurate statement is: Europe uses fluoride in different ways. Some European countries deliberately chose to fluoridate salt rather than water, and they do benefit from fluoride’s effects. In areas where neither water nor salt is fluoridated, other measures (such as comprehensive dental programs or naturally occurring fluoride) are often in place. It’s also worth noting that where Europe has tried fluoridation, it worked. For example, the former East Germany had extensive water fluoridation in the 1980s and saw significant reductions in decay; after reunification, they switched to salt fluoridation due to legal/philosophical preferences, not because of a lack of efficacy.
In terms of safety, many European scientific reviews (e.g., the UK’s Medical Research Council 2002 report and the EU SCHER 2011 report) echoed the same conclusions as those in the U.S. and elsewhere: no evidence of systemic harm from fluoridation. Their decisions not to implement it widely often hinged on social acceptability and the availability of other fluoride vehicles, rather than a damning safety indictment. For instance, Sweden’s government in the 1970s decided against fluoridation largely on philosophical grounds (preferring individual choice), but its national academy of sciences had found it was safe and effective. Thus, invoking Europe is more a debate about policy approach than about science. Public health experts can acknowledge that there is more than one way to skin the cat of preventing cavities – fluoridated water is one proven way; others include fluoridated salt or well-funded preventive dentistry. The U.S. chose the water route and has greatly benefited from it. Countries that didn’t go that route had to ensure fluoride came in through other means or accept higher levels of decay. In fact, a few non-fluoridated, high-income countries initially saw slower declines in dental decay than fluoridated ones did, until fluoride toothpaste became ubiquitous.
The key takeaway: Fluoridation is not “unnecessary” in the U.S. context just because other countries use different methods.
If we removed fluoride from all U.S. water tomorrow, cavity rates would almost certainly rise, particularly in the most vulnerable groups (as historical and contemporary case studies suggest). Europe’s example doesn’t prove fluoridation is useless; it only shows that the same end (reducing cavities) can sometimes be achieved by alternate strategies, albeit with their own trade-offs (for example, salt fluoridation relies on consistent use of fluoridated salt and reaches those who use salt at home but not necessarily all processed foods, etc.). Many public health experts actually encourage fluoridated salt in countries where water fluoridation isn’t feasible – one method isn’t inherently superior; it depends on context. The U.S. has a highly centralized water distribution in many cities, making water fluoridation a convenient and equitable method. And it has worked: Americans’ decayed and missing teeth have dropped dramatically since the mid-20th century, with fluoridation cited as a major factor.
The lack of water fluoridation in some countries should not be misinterpreted as a condemnation of fluoride’s effectiveness or safety. It is usually due to policy preference and the presence of other fluoride delivery systems. Dental health improvements worldwide owe a debt to fluoride in one form or another. The U.S. experience – supported by countless studies and the endorsement of every major medical and dental organization – demonstrates that water fluoridation is a safe, effective, and efficient way to prevent tooth decay on a broad scale. Until an easier, cheaper, and equally effective alternative comes along, fluoridation remains a cornerstone of public health dentistry in America. Other countries’ choices do not negate the science; if anything, they offer opportunities to learn about different public health approaches, all aimed at the same goal: reducing the burden of dental disease.
Wrapping up
Water fluoridation in the United States stands as a remarkable intersection of science, policy, and public trust. From its beginnings in the 1940s as an innovative experiment to its present status as a routine public health practice reaching over 200 million Americans, fluoridation has repeatedly proven its worth by making our teeth stronger and our dental bills smaller. It is often cited as one of the great public health achievements of the 20th century, right alongside vaccinations and clean water reforms, precisely because it exemplifies the power of prevention. The historical record shows a clear trajectory: cavities and tooth loss were rampant ailments of American life a century ago, and today they are far less common, thanks in no small part to fluoride.
Yet, as we have detailed, fluoridation has also been a lightning rod for fear and misinformation. In a sense, it is a case study in the challenges of science communication. A simple, common-sense idea – adjusting a natural mineral in water to improve health – became the subject of bizarre conspiracy theories and public debates that have lingered for generations. For public health professionals, this underscores the importance of transparency, community engagement, and continued research.
We must acknowledge people’s concerns, but also clearly present the substantial evidence supporting fluoridation’s safety and efficacy. Every claim deserves a response rooted in facts: No, it’s not poison at the dose we use; yes, major studies have looked for cancer links and found none; no, it’s not a communist mind-control trick; yes, it does reduce cavities significantly; and no, we’re not behind the times – we’re using a method that works in our context, just as others use fluoride in other ways.
The endurance of fluoridation myths can be frustrating, but it also offers an opportunity. It allows health professionals to engage with the public on broader topics of scientific literacy –>how we know what we know and why consensus matters. In the face of any misinformation (about fluoride, vaccines, or other public health measures), the strategy is similar: listen respectfully, explain the evidence, cite reputable sources, and put risks and benefits in perspective. As we’ve shown, authoritative bodies from the CDC to the American Dental Association to the World Health Organization have consistently reaffirmed that community water fluoridation is a prudent, effective public health policy. Over 75 years, millions of Americans have lived healthier lives with fewer cavities and without the dire health consequences opponents predicted. Those are the facts.
Public health is fundamentally about building trust that officials are guided by the best evidence and have the community’s well-being at heart. The fluoridation story, when properly told, is one of scientific triumph and good governance: a case in which an observation led to research, which in turn led to a preventive innovation that benefited society. By remaining open about the science and diligent in addressing concerns, we can maintain public trust in this measure. And by being vigilant (continuing research on fluoride’s effects and adjusting policies when new credible evidence calls for it), we demonstrate that public health policies are not dogmas but evolving practices designed to maximize health and safety.
In conclusion, water fluoridation remains a safe, smart, and cost-effective investment in our population’s health. The conspiracy theories that swirl around it have no real teeth – they crumble under the scrutiny of scientific evidence. As professionals in dentistry, epidemiology, and health communication, we should feel confident in championing fluoridation as a success story while compassionately debunking persistent myths. By understanding both the science and the sociology around fluoridation, we can better communicate why this public health policy deserves our support – and why, in the grand scheme of things, it’s something to smile about.
References
- McGill Office for Science and Society – The Fluoride Controversy (2019).
- Centers for Disease Control and Prevention – Community Water Fluoridation: 70 Years of Success (2015).
- CDC – Timeline for Community Water Fluoridation.
- NIH National Institute of Dental and Craniofacial Research – The Story of Fluoridation.
- American Public Health Association – Policy Statement: Community Water Fluoridation in the U.S. (2013).
- American Cancer Society – Water Fluoridation and Cancer Risk (2020).
- The Untold Story of Fluoridation: Revisiting the Changing Perspectives. J. Int. Soc. Prevent. Comm. Dent. (2018).
- Columbia University – State of the Planet: “Fluoridation of Water: Communist Conspiracy or Genuine Threat?” (2010).
- APHA – Community Water Fluoridation page.
- Office of Science & Society, McGill – Analysis of recent fluoride/IQ studies (2019).